

Your Filing and Shelving Experts!
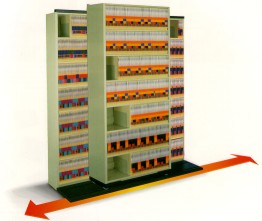
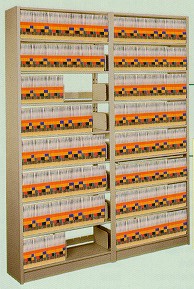
- We can maximize your Filing/Shelving/Storage needs - From design to installation we can help!Shelving – Rotating Shelving – High Density Mobile Shelving - Side to Side Shelving – Retractable Shelving - Open Shelf Shelving - Storage/Archival Shelving - Rollok Door

.jpg)

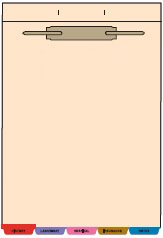
File Folders


AAK Filing System


Our most popular filing system is the AAK Filing® System. This filing system is used by thousands of offices around the world! The AAK Filing® System is a colored based filing system that eliminates misfiles and speeds up filing by 80% over standard alphabetical filing systems. Let Allied Systems Products help customize and convert your filing system today.

Our team of lead installers will get your project done on time, on budget, and with the attention to detail you expect. Whether you need a few chairs delivered, or an entire office furniture installation, Allied Systems Products can help.